为重症救治赋能
为患者康复加速

登录
注册
登录方式
方式一:
PC端网页:www.rccrc.cn
输入账号密码登录,可将此网址收藏并保存密码方便下次登录
方式二:
手机端网页:www.rccrc.cn
输入账号密码登录,可将此网址添加至手机桌面并保存密码方便下次登录
方式三:
【重症肺言】微信公众号
输入账号密码登录
注:账号具有唯一性,即同一个账号不能在两个地方同时登录。
孟广平 吉林大学第二医院 发布于2024-05-17 浏览 1285
 收藏
收藏
单位:吉林大学第二医院呼吸与危重症医学科
01
CIP潜在的危险因素[5]主要有:①年龄:患者年龄多在70岁以上[6];②性别:女性发病率高于男性[7];③吸烟史:吸烟者比不吸烟者更容易发生[8];④既往肺部疾病史:有间质性肺疾病、慢性阻塞性肺疾病、哮喘、气胸、胸腔积液和肺纤维化病史患者CIP发生率高;⑤肿瘤组织学类型:相较于腺癌,鳞癌患者发生CIP的概率更高;⑥PD-1抑制剂:使用PD-1/PD-L1抑制剂会增加CIP的发生风险[9];⑦联合治疗:接受联合治疗的患者CIP发生率增加了2~3倍,抗生素和免疫抑制药物是ICIs治疗后肺部感染的主要危险因素;⑧既往放射治疗病史:放射治疗与免疫疗法存在协同作用[10]。
02
目前CIP的发病机制尚未得到明确阐述,仍需深入探究[10]。可能与下述情况有关:①T细胞对肿瘤和正常组织中表达的交叉抗原的活性增加;②自身抗体和炎性细胞因子水平升高:CIP患者血浆抗CD74水平升高;CIP的非小细胞癌患者IL-6、IL-17A、IL-35、CRP、PCT、SP-D和KL-6升高;③增强补体介导的炎症[11]。
03
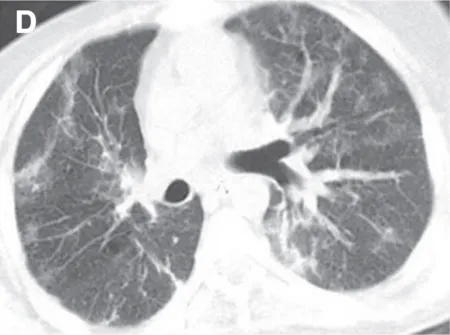
(2)隐源性机化性肺炎(COP):是NSCLC中最常见的CIP类型,双侧多灶性实变,周围和下肺分布,伴有GGO和网状阴影[17]。
还可以表现为机化性肺炎(OP),反向环礁或晕征,被认为是CIP中OP的相对特殊特征[18]。
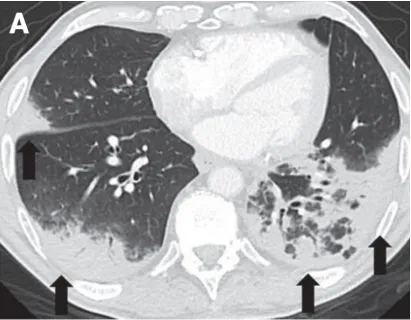
(3)非特异性间质性肺炎(NSIP):是CIP第二常见的报道类型,通常表现为肺下叶GGO和网状结构[17]。
(7)未分类型。
4. 病理表现[20,21]
CIP的病理表现主要为:①嗜酸性粒细胞浸润;②肉芽肿性炎症;③肺泡实质伴成纤维细胞灶;④肺泡间隔轻度胶原扩张;⑤非特异性慢性炎症;⑥不典型细胞。
04
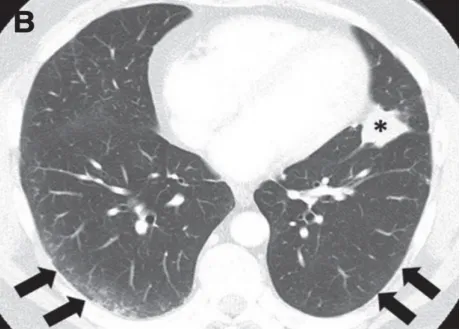
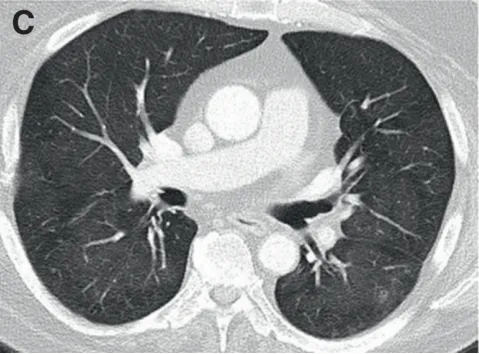
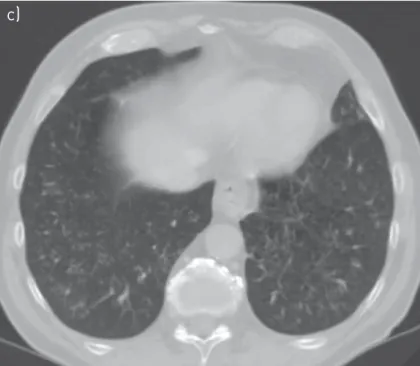
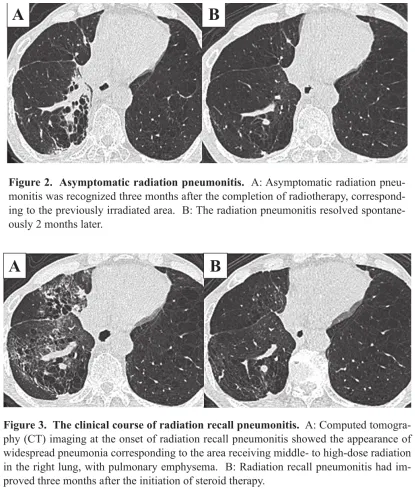
RIP是一种放射性肺损伤的早期表现,也是CIP的鉴别诊断难点[25-27]。两种疾病的相似之处在于:①发病时间接近(1~3个月);②相似的影像特征(GGO和弥漫性模糊影);③共同的病理特征(淋巴细胞性肺泡炎);④相同的一线治疗方案:糖皮质激素。不同之处在于二者的病变部位存在差异,RIP主要存在于放射性区域,CIP多发生在放射治疗下降剂量以外或低剂量区。
05
托珠单抗是一种IL-6抑制剂,已被用于治疗风湿性免疫相关不良反应[31]。一份病例报告显示,一名NSCLC和CIP患者在接受托珠单抗额外治疗后症状显著缓解[32]。然而,是否应该将托珠单抗作为治疗激素难治性免疫相关不良反应患者的二线药物的选择仍未确定,因为该方法缺乏与其他二线药物的比较。
06
大多数CIP患者在接受糖皮质激素治疗后恢复良好。然而,由于继发感染、肿瘤进展或免疫抑制剂治疗无效,一些患者的预后仍然很差,约1/4的CIP患者会复发。CIP治愈后,临床医生将面临是否重新开启ICIs治疗的决定。大多数患者在重启免疫治疗后没有复发。诊断为3级或4级CIP的患者通常永久停止ICIs治疗,因此,重复使用ICIs治疗的报道主要发生在最初的1级或2级CIP患者中,其复发率从17%至30%不等[33]。复发性肺炎的类型、受累部位和严重程度可能与最初的表现不同。尽管在美国临床肿瘤学实践指南中没有具体说明,但复发性肺炎的治疗方法通常与首次发生时的治疗方法相似。
07 [1] Kalisz K R, Ramaiya N H, Laukamp K R, et al. Immune Checkpoint Inhibitor Therapy-related Pneumonitis: Patterns and Management[J]. Radiographics, 2019, 39(7):1923-1937. [2] Shannon V R. Pneumonitis Associated With Immune Checkpoint Inhibitors Among Patients With non-Small Cell Lung Cancer[J]. Curr Opin Pulm Med, 2020, 26(4):326-340. [3] Lin X, Lu X, Luo G S, et al. Progress in PD-1/PD-L1 Pathway Inhibitors: From Biomacromolecules to Small Molecules[J]. Eur J Medicinal Chem, 2020, 186:111876. [4] Suresh K, Naidoo J, Lin C T, et al. Immune Checkpoint Immunotherapy for Non-Small Cell Lung Cancer: Benefits and Pulmonary Toxicities[J]. Chest, 2018, 154(6):1416-1423. [5] Zhang Q, Tang L, Zhou Y, et al. Immune Checkpoint Inhibitor-Associated Pneumonitis in Non-Small Cell Lung Cancer: Current Understanding in Characteristics, Diagnosis, and Management[J]. Front Immunol, 2021, 12:663986. [6] Cho J Y, Kim J, Lee J S, et al. Characteristics, Incidence, and Risk Factors of Immune Checkpoint Inhibitor-Related Pneumonitis in Patients With Non-Small Cell Lung Cancer[J]. Lung Cancer, 2018, 125:150-156. [7] Suresh K, Khinh Ranh V, et al. Pneumonitis in Non-Small Cell Lung Cancer Patients Receiving Immune Checkpoint Immunotherapy: Incidence and Risk Factors[J]. J Thoracic Oncol, 2018, 13(12):1930-1939. [8] Voong K R, Hazell S, Hu C, et al. Receipt of Chest Radiation and Immune-Related Pneumonitis in Patients With NSCLC Treated With Anti-PD-1/PD-L1[J]. J Thoracic Oncol, 2017, 12(11):S1837-7. [9] van Eeden R, Rapoport B L, Smit T, et al. Tuberculosis Infection in a Patient Treated With Nivolumab for Non-small Cell Lung Cancer: Case Report and Literature Review[J]. Front Oncol, 2019, 9:659. [10] Zhai X, Zhang J, Tian Y, et al. The Mechanism and Risk Factors for Immune Checkpoint Inhibitor Pneumonitis in non-Small Cell Lung Cancer Patients[J]. Cancer Biol Med, 2020, 17(3):599-611. [11] Caturegli P, Di Dalmazi G, Lombardi M, et al. Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights Into Pathogenesis From an Autopsy Series[J]. Am J Pathol, 2016, 186(12):3225-3235. [12] Nishino M, Ramaiya N H, Awad M M, et al. PD-1 inhibitor-related pneumonitis in advanced cancer patients: radiographic patterns and clinical course[J]. Clin Cancer Res, 2016, 22(24):6051-6060. [13] Kato T, Masuda N, Nakanishi Y, et al. Nivolumab-induced interstitial lung disease analysis of two phase II studies patients with recurrent or advanced non-small-cell lung cancer[J]. Lung Cancer, 2017, 104:111-118. [14] Naidoo J, Wang X, Woo K M, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy[J]. J Clin Oncol, 2017, 35(7):709-717. [15] Delaunay M, Cadranel J, Lusque A, et al. Immune-checkpoint inhibitors associated with interstitial lung disease in cancer patients[J]. Eur Respir J, 2017, 50(2):1700050. [16] Gounant V, Brosseau S, Naltet C, et al. Nivolumab-Induced Organizing Pneumonitis in a Patient With Lung Sarcomatoid Carcinoma[J]. Lung Cancer, 2016, 99:162-165. [17] Nishino M, Hatabu H, Hodi F S, et al. Drug-Related Pneumonitis in the Era of Precision Cancer Therapy[J]. JCO Precis Oncol, 2017, 1:PO.17.00026. [18] Fragkou P, Souli M, Theochari M, et al. A Case of Organizing Pneumonia (OP) Associated with Pembrolizumab[J]. Drug Target Insights, 2016, 10:9-12. [19] Itamura H, Ohguri T, Yahara K, et al. Pembrolizumab-induced Radiation Recall Pneumonitis After the Resolution of Typical Asymptomatic Radiation Pneumonitis[J]. J UOEH, 2020, 42(3):261-266. [20] Li H, Ma W, Yoneda KY, et al. Severe Nivolumab-Induced Pneumonitis Preceding Durable Clinical Remission in a Patient With Refractory, Metastatic Lung Squamous Cell Cancer: A Case Report[J]. J Hematol Oncol, 2017, 10(1):64. [21] Kanai O, Nakatani K, Fujita K, et al. Concurrence of Nivolumab-Induced Interstitial Lung Disease and Cancer Invasion[J]. Respirol Case Rep, 2017, 5(6):e00257. [22] Wang Y N, Lou D F, Li D Y, et al. Elevated levels of IL-17A and IL-35 in plasma and bronchoalveolar lavage fluid are associated with checkpoint inhibitor pneumonitis in patients with non-small cell lung cancer[J]. Oncol Lett, 2020, 20(1):611-622. [23] Colella S, Haentschel M, Shah P, et al. Transbronchial lung cryobiopsy in interstitial lung diseases: best practice[J]. Respiration, 2018, 95(6):383-391. [24] Johnson D B, Balko J M, Compton M L, et al. Fulminant Myocarditis With Combination Immune Checkpoint Blockade[J]. N Engl J Med, 2016, 375(18):1749-1755. [25] Sekine I, Sumi M, Ito Y, et al. Retrospective Analysis of Steroid Therapy for Radiation-Induced Lung Injury in Lung Cancer Patients[J]. Radiother Oncol, 2006, 80(1):93-97. [26] Chen Y, Williams J, Ding I, et al. Radiation Pneumonitis and Early Circulatory Cytokine Markers[J]. Semin Radiat Oncol, 2002, 12(1 Suppl 1):26-33. [27] Chuzi S, Tavora F, Cruz M, et al. Clinical Features, Diagnostic Challenges, and Management Strategies in Checkpoint Inhibitor-Related Pneumonitis[J]. Cancer Manag Res, 2017, 9:207-213. [28] Gomatou G, Tzilas V, Kotteas E, et al. Immune Checkpoint Inhibitor-Related Pneumonitis[J]. Respiration, 2020, 99(11):932-942. [29] Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2017, 28(suppl_4):iv119-iv142. [30] Brahmer J R, Lacchetti C, Schneider B J, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline[J]. J Clin Oncol, 2018, 36(17):1714-1768. [31] Cappelli L C, Gutierrez A K, Baer A N, et al. Inflammatory Arthritis and Sicca Syndrome Induced by Nivolumab and Ipilimumab[J]. Ann Rheum Dis, 2017, 76(1):43-50. [32] Naqash A R, Yang L V, Sanderlin E J, et al. Interleukin-6 as One of the Potential Mediators of Immune-Related Adverse Events in Non-Small Cell Lung Cancer Patients Treated With Immune Checkpoint Blockade: Evidence From a Case Report[J]. Acta Oncol, 2018, 57(5):705-708. [33] Rashdan S, Minna J D, Gerber D E. Diagnosis and Management of Pulmonary Toxicity Associated With Cancer Immunotherapy[J]. Lancet Respir Med, 2018, 6(6):472-478.
 后可发表评论
后可发表评论



友情链接
联系我们
 公众号
公众号
 客服微信
客服微信