为重症救治赋能
为患者康复加速

登录
注册
登录方式
方式一:
PC端网页:www.rccrc.cn
输入账号密码登录,可将此网址收藏并保存密码方便下次登录
方式二:
手机端网页:www.rccrc.cn
输入账号密码登录,可将此网址添加至手机桌面并保存密码方便下次登录
方式三:
【重症肺言】微信公众号
输入账号密码登录
注:账号具有唯一性,即同一个账号不能在两个地方同时登录。
张立明 重庆市人民医院 发布于2024-05-23 浏览 784
 收藏
收藏
作者:张立明
01
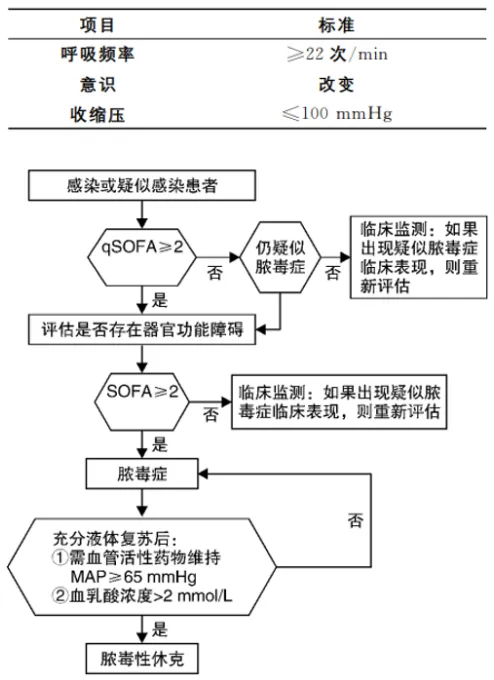
感染性休克又称脓毒性休克。脓毒症(sepsis)是指因感染引起的宿主反应失调导致的危及生命的器官功能障碍,而脓毒性休克(sepsis shock)是指脓毒症合并严重的循环、细胞和代谢功能紊乱。提到感染性休克,不得不提及“Sepsis”定义的变迁。Sepsis 1.0的定义是感染或高度可疑感染+全身炎症反应综合征,但这一定义过于宽泛,对脓毒症的诊断可能会存在一些误差。Sepsis 2.0在1.0的基础上增加了20余条诊断指标,但这一诊断标准过于复杂,不适于临床应用。因此,2016年更新了Sepsis 3.0,将脓毒症定义为感染或可疑感染+SOFA评分≥2分,该定义的特点是纳入了“器官功能损伤”的概念,并且SOFA评分≥2分能够更好地评估患者的预后。
《中国脓毒症/脓毒性休克急诊治疗指南(2018)》[1]中给出了脓毒症和脓毒性休克的临床诊断流程。首先,感染或疑似感染患者进行qSOFA评分,如果qSOFA评分≥2分,再进行SOFA评分,如果SOFA评分≥2分,则诊断脓毒症。在脓毒症诊断基础上,如果经过了充分的液体复苏,仍然需要使用血管活性药物,或者血乳酸水平仍>2 mmol/L,则诊断脓毒性休克。
2018年Lancet 发表的“脓毒症和脓毒性休克”一文中提到在脓毒症的病因中,社区感染占80%,医院感染占20%;在来源部位中,肺部占64%,腹部占20%,血流占15%,肾及泌尿系占14%;病原微生物方面,革兰氏阴性菌和革兰氏阳性菌大体相当,常见的病原菌主要有金黄色葡萄球菌、假单胞菌、大肠杆菌[2]。
02
感染性休克导致的循环高流量与组织缺氧主要是因为:①血流分布的异常:阻力血管舒缩调节功能受损,动-静脉短路开放,有待进一步证实;②线粒体功能不全:细菌毒素、炎症介质影响,正常或高灌注下细胞缺氧[5]。
03
2018年发表在Intensive Care Med 的一项荟分析纳入了6361例脓毒症患者,结果发现与对照组相比,经胸超声组28天死亡率明显改善[12]。2022年的一项RCT研究显示,使用超声目标导向治疗的染性休克患者在6小时乳酸改善率、12小时和24小时总累计液体输注量和液体平衡方面具有显著优势[13]。
04 05 [1] 中国医师协会急诊医师分会, 中国研究型医院学会休克与脓毒症专业委员会. 中国脓毒症/脓毒性休克急诊治疗指南(2018)[J]. 中国急救医学, 2018, 38(9):741-756. [2] Cecconi M, Evans L, Levy M, et al. Sepsis and septic shockp[J]. Lancet, 2018, 392(10141):75-87. [3] Font M D, Thyagarian B, Khaa A K. Sepsis and Septic Shock-Basics of diagnosis, pathophysiology and clinical decision making[J]. Med Clin Noth Am, 2020, 104(4):573-585. [4] Russell J A, Rush B, Boyd J. Pathophysiology of Septic Shock[J]. Crit Care Clin, 2018, 34(l):43-61. [5] Jacobi J. The pathophysiology of sepsis-2021 update: Pat 1, immunology and coagulopathy leading to endothelial injury[J]. Am J Heath Syst Pharm, 2022, 79(5):329-337. [6] Hemandez G, Ospina-Tascon G A, Damiani L P, et al. Efeet of a Resuscitation Strategy Tarzeting Peripherd Perhusion Status vs Senm Lactate levels on 28-DayMortality Amone Patients With Sentic Shock: The ANDROMEDA-SHOCK Randomized Cinical Tral[J]. JAMA, 2019, 321(7):654-664. [7] Rajaram S S, Desai N K, Kalra A, et al. Pulmonary artery catheters for adult patients in intensive care[J]. Cochrane Database Syst Rev, 2013, 2013(2):CD003408. [8] Wang B, Cai L, Lin B, et al. Efect of Puse ndicator Contimous Cardiac Output Monitoring on Sepsie Shock Patients: A Meta-Analysis[J]. Comput Math Methods Med, 2022, 2022:8604322. [9] Dai R, Zhang X, Wang H, et al. [Clinical value of point of care ultrasound on cardiac output and volume responsiveness in patients with septic shock][J]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021, 33(12):1479-1483. [10] Sanders M, Servaas S, Slagt C. Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis[J]. J Clin Monit Comput, 2020, 34(3):433-460. [11] Mansfield R C, Kaza N, Charalambous A, et al. Cardiac Output Measurement in Neonates and Children Using Noninvasive Electrical Bioimpedance Compared With Standard Methods: A Systematic Review and Meta-Analysis[J]. Crit Care Med, 2022, 50(1):126-137. [12] Feng M, McSparron J I, Kien D T, et al. Transthoracic echocardiography and mortality in sepsis: analysis of the MIMIC-III database[J]. Intensive Care Med, 2018, 44(6):884-892. [13] Yu K, Zhang S, Chen N, et al. Critical care ultrasound goal-directed versus early goal-directed therapy in septic shock[J]. Intensive Care Med, 2022, 48(1):121-123. [14] Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021[J]. Crit Care Med, 2021, 49(11):e1063-e1143. [15] Rygård S L, Butler E, Granholm A, et al. Low-dose corticosteroids for adult patients with septic shock: a systematic review with meta-analysis and trial sequential analysis[J]. Intensive Care Med, 2018, 44(7):1003-1016. [16] Dellinger R P, Bagshaw S M, Antonelli M, et al. Effect of Targeted Polymyxin B Hemoperfusion on 28-Day Mortality in Patients With Septic Shock and Elevated Endotoxin Level: The EUPHRATES Randomized Clinical Trial[J]. JAMA, 2018, 320(14):1455-1463. [17] STARRT-AKI Investigators, Canadian Critical Care Trials Group, Australian and New Zealand Intensive Care Society Clinical Trials Group, et al. Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury[J]. N Engl J Med, 2020, 383(3):240-251. [18] Welte T, Dellinger R P, Ebelt H, et al. Efficacy and safety of trimodulin, a novel polyclonal antibody preparation, in patients with severe community-acquired pneumonia: a randomized, placebo-controlled, double-blind, multicenter, phase II trial (CIGMA study)[J]. Intensive Care Med, 2018, 44(4):438-448. [19] Cui J, Wei X, Lv H, et al. The clinical efficacy of intravenous IgM-enriched immunoglobulin (pentaglobin) in sepsis or septic shock: a meta-analysis with trial sequential analysis[J]. Ann Intensive Care, 2019, 9(1):27. 硕士,副主任医师 重庆市人民医院呼吸与危重症医学科重症组组长 重庆市医师协会呼吸医师分会呼吸危重症与呼吸治疗专业委员会委员 重庆市基层呼吸工作委员会委员 擅长各种人工气道、血管通路建立,机械通气,血流动力学监测及慢重症呼吸康复
*本文根据“呼吸危重症菁英秀”第二十期专题视频整理,感谢张立明医师予以审核。
 后可发表评论
后可发表评论



友情链接
联系我们
 公众号
公众号
 客服微信
客服微信