为重症救治赋能
为患者康复加速

登录
注册
登录方式
方式一:
PC端网页:www.rccrc.cn
输入账号密码登录,可将此网址收藏并保存密码方便下次登录
方式二:
手机端网页:www.rccrc.cn
输入账号密码登录,可将此网址添加至手机桌面并保存密码方便下次登录
方式三:
【重症肺言】微信公众号
输入账号密码登录
注:账号具有唯一性,即同一个账号不能在两个地方同时登录。
夏金根 国家呼吸医学中心 中日友好医院 呼吸与危重症医学科 发布于2023-04-26 浏览 1831
 收藏
收藏
单位:国家呼吸医学中心 中日友好医院 呼吸与危重症医学科
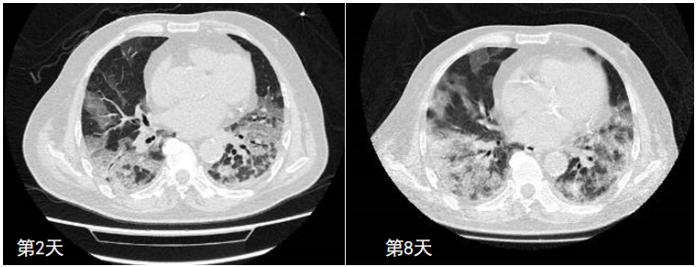
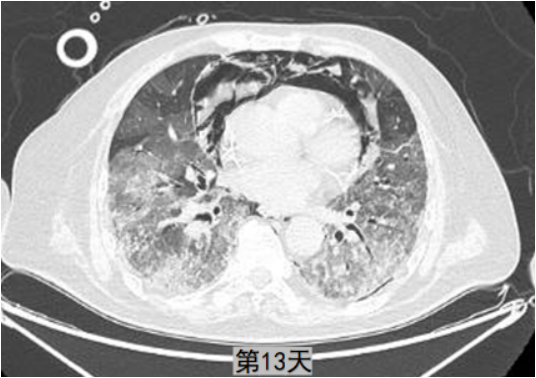
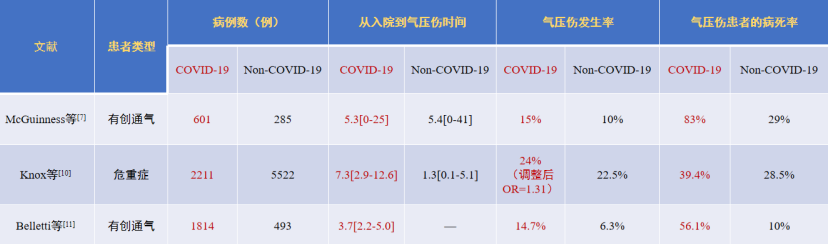
一、病例 二、导致COVID-19患者气压伤的原因 COVID-19患者气压伤发生率为何如此之高?我们分析这可能与下列因素有关:①患者因素:COVID-19 ARDS发生率高?COVID-19疾病本身特性?病变的不均一性?②人为因素:呼吸机参数设置问题?③医疗资源的限制。其中,COVID-19 ARDS发生率增加是重要原因。据统计,在COVID-19期间ARDS人数较非COVID-19期间增加了将近20倍[12]。此外,在后COVID-19时代,即使COVID-19患病人数下降,ARDS的长期损害预计也会增加[13]。因此,ARDS的疾病负担显著增加。一项全球文献调查显示,在ICU中,COVID-19患者ARDS的发生率可以达到75%(47%~100%),病死率高达45%(20%~89%)[14]。由于ARDS本身导致肺组织病变不均一,更易出现气压伤。 一项研究提示我们COVID-19相关ARDS与普通ARDS是有区别的。虽然该研究纳入患者的呼吸机压力水平偏高,但仍然在肺保护性通气策略的范围之内,然而COVID-19与非COVID-19患者气压伤发生率分别为13.6%和1.9%。将所有气压伤(包括纵隔气肿和皮下气肿)进行队列分析发现,发生气压伤与未发生气压伤的COVID-19患者呼吸机参数设定是相同的,二者之间没有区别[16]。所以“lung frailty”可能是很重要的一个因素,如同SARS和MERS,尽管报道不多,但仅有的一些文献会发现其气压伤的发生率仍然可以达到20%。 三、COVID-19患者气压伤的预防
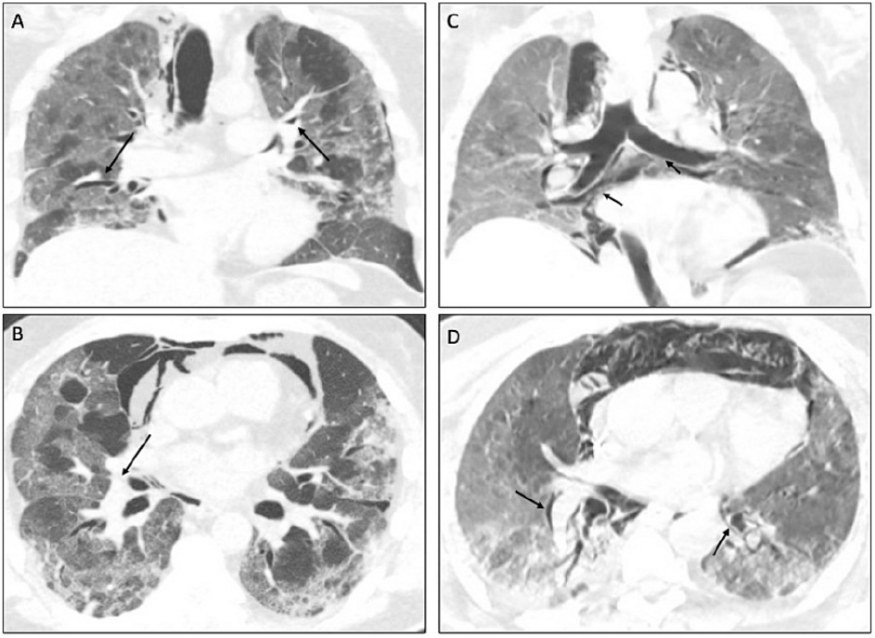
对于COVID-19患者,如果PEEP从0增加至10或15 cmH2O,患者的氧合的确改善,但从呼吸力学的角度分析,结果并非如此,增加PEEP后,虽然氧合指数增加,但肺顺应性下降,PaCO2也降低。通过胸部CT可以发现,增加PEEP后,复张的肺组织很多,但过度充气的肺组织也会增加,当增加PEEP时,复张的肺容积每增加1 ml,同时会伴随1.1 ml肺组织的过度充气。所以,高PEEP可能并不适合COVID-19患者[18]。
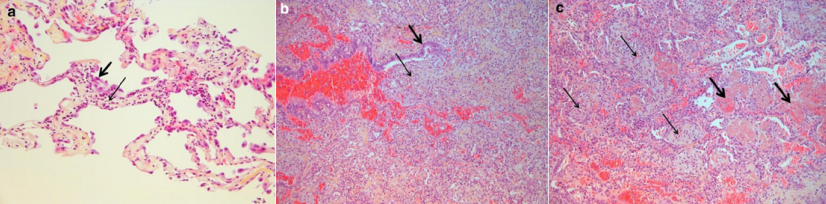
2000年一项COVID-19患者的尸检报告发现,在6例死亡患者中有5例出现了机化性肺炎,在肺泡腔及细支气管中都填充着纤维素样渗出[19],此时增加PEEP并不会产生任何作用,相反,正常肺泡过度膨胀,患者气压伤和呼吸机相关性肺损伤的发生率显著增加。
注:a. 肺泡壁被大量淋巴细胞浸润和水肿(细箭头);b. 支气管内的松散结缔组织(细箭头);c. 肺泡管内的组织性肺炎(细箭头)与纤维蛋白球(粗箭头)共存。
四、小结
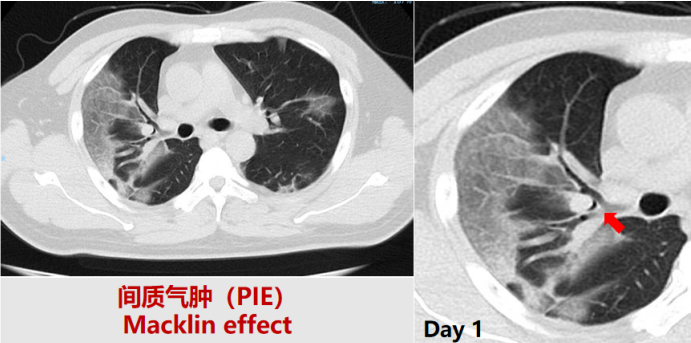
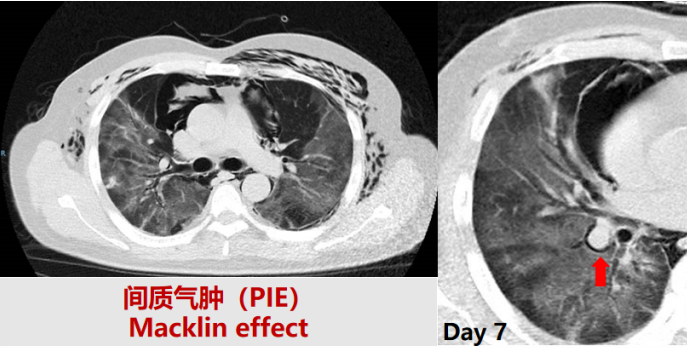
在临床工作中,一定要警惕重症COVID-19患者的气压伤。COVID-19患者的气压伤发生率高于非COVID-19患者,其可能的影响因素包括原发病因素、呼吸机参数因素及医疗资源受限因素。预防气压伤的发生需要考虑:①肺保护性通气策略:尽可能降低Pplat、驱动压;②慎用过高PEEP(>10~12 cmH2O);③避免过强的自主呼吸:VT<8 ml/kg,Δpes<10 cmH2O,Ptp<20 cmH2O等;④关注早期气压伤征象:Macklin effect(PIE);⑤氧合改善不明显应及时考虑俯卧位通气和ECMO。
参考文献 [1] Gammon R B, Shin M S, Buchalter S E. Pulmonary barotrauma in mechanical ventilation. Patterns and risk factors[J]. Chest, 1992, 102(2):568-572. [2] Gattinoni L, Bombino M, Pelosi P, et al. Lung structure and function in different stages of severe adult respiratory distress syndrome[J]. JAMA, 1994, 271(22):1772-1779. [3] Brower R G, Lanken P N, MacIntyre N, et al. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome[J]. N Engl J Med, 2004, 351(4):327-336. [4] Meade M O, Cook D J, Guyatt G H, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial[J]. JAMA, 2008, 299(6):637-645. [5] Mercat A, Richard J C, Vielle B, et al. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial[J]. JAMA, 2008, 299(6):646-655. [6] Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators; Cavalcanti AB, Suzumura ÉA, et al. Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome: A Randomized Clinical Trial[J]. JAMA, 2017, 318(14):1335-1345. [7] McGuinness G, Zhan C, Rosenberg N, et al. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation[J]. Radiology, 2020, 297(2):E252-E262. [8] Shrestha D B, Sedhai Y R, Budhathoki P, et al. Pulmonary barotrauma in COVID-19: A systematic review and meta-analysis[J]. Ann Med Surg (Lond), 2022, 73:103221. [9] Umbrello M, Venco R, Antonucci E, et al. Incidence, clinical characteristics and outcome of barotrauma in critically ill patients with COVID-19: a systematic review and meta-analysis[J]. Minerva Anestesiol, 2022, 88(9):706-718. [10] Knox D B, Brunhoeber A, Peltan I D, et al. Comparison of radiographic pneumothorax and pneumomediastinum in COVID-19 vs. non-COVID-19 acute respiratory distress syndrome[J]. Intensive Care Med, 2022, 48(11):1648-1651. [11] Belletti A, Todaro G, Valsecchi G, et al. Barotrauma in Coronavirus Disease 2019 Patients Undergoing Invasive Mechanical Ventilation: A Systematic Literature Review[J]. Crit Care Med, 2022, 50(3):491-500. [12] Wick K D, McAuley D F, Levitt J E, et al. Promises and challenges of personalized medicine to guide ARDS therapy[J]. Crit Care, 2021, 25(1):404. [13] Palakshappa J A, Krall J T W, Belfield L T, et al. Long-Term Outcomes in Acute Respiratory Distress Syndrome: Epidemiology, Mechanisms, and Patient Evaluation[J]. Crit Care Clin, 2021, 37(4):895-911. [14] Tzotzos S J, Fischer B, Fischer H, et al. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: a global literature survey[J]. Crit Care, 2020, 24(1):516. [15] Botta M, Tsonas AM, Pillay J, et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): a national, multicentre, observational cohort study[J]. Lancet Respir Med, 2021, 9(2):139-148. [16] Lemmers D H L, Abu Hilal M, Bnà C, et al. Pneumomediastinum and subcutaneous emphysema in COVID-19: barotrauma or lung frailty?[J]. ERJ Open Res, 2020, 6(4):00385-2020. [17] Knox D B, Brunhoeber A, Peltan I D, et al. Comparison of radiographic pneumothorax and pneumomediastinum in COVID-19 vs. non-COVID-19 acute respiratory distress syndrome[J]. Intensive Care Med, 2022 , 48(11):1648-1651. [18] Protti A, Santini A, Pennati F, et al. Lung Response to a Higher Positive End-Expiratory Pressure in Mechanically Ventilated Patients With COVID-19[J]. Chest, 2022, 161(4):979-988. [19] Copin M C, Parmentier E, Duburcq T, et al. Time to consider histologic pattern of lung injury to treat critically ill patients with COVID-19 infection[J]. Intensive Care Med, 2020, 46(6):1124-1126. [20] Grasselli G, Greco M, Zanella A, et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy[J]. JAMA Intern Med, 2020, 180(10):1345-1355. [21] Vetrugno L, Castaldo N, Fantin A, et al. Ventilatory associated barotrauma in COVID-19 patients: A multicenter observational case control study (COVI-MIX-study)[J]. Pulmonology, 2022 Nov 24:S2531-0437(22)00260-4. [22] Grieco D L, Maggiore S M, Roca O, et al. Non-invasive ventilatory support and high-flow nasal oxygen as first-line treatment of acute hypoxemic respiratory failure and ARDS[J]. Intensive Care Med, 2021, 47(8):851-866. [23] Esnault P, Cardinale M, Hraiech S, et al. High Respiratory Drive and Excessive Respiratory Efforts Predict Relapse of Respiratory Failure in Critically Ill Patients with COVID-19[J]. Am J Respir Crit Care Med, 2020, 202(8):1173-1178. [24] Coppola S, Chiumello D, Busana M, et al. Role of total lung stress on the progression of early COVID-19 pneumonia[J]. Intensive Care Med, 2021, 47(10):1130-1139. [25] Elabbadi A, Urbina T, Berti E, et al. Spontaneous pneumomediastinum: a surrogate of P‑SILI in critically ill COVID‑19 patients[J]. Crit Care, 2022, 26(1):350. [26] Maccarrone V, Liou C, D'souza B, et al. The Macklin effect closely correlates with pneumomediastinum in acutely ill intubated patients with COVID-19 infection[J]. Clin Imaging, 2023, 97:50-54. [27] Paternoster G, Bertini P, Belletti A, et al. Venovenous Extracorporeal Membrane Oxygenation in Awake Non-Intubated Patients With COVID-19 ARDS at High Risk for Barotrauma[J]. J Cardiothorac Vasc Anesth, 2022, 36(8 Pt B):2975-2982. 作者简介 中日友好医院呼吸中心呼吸与危重症医学科副主任呼吸治疗师 中华医学会呼吸病学分会呼吸治疗学学组委员 中国医师协会呼吸医师分会呼吸相关职业发展工作委员会委员 中国医学装备协会呼吸病学装备专业委员会第一届委员 中国病理生理学会危重病专业委员会第一届呼吸治疗学组委员 中国康复医学会呼吸康复委员会委员 中国医学救援协会重症医学分会理事会理事
 后可发表评论
后可发表评论

相关推荐
1
詹庆元教授|关于制作「重症COVID-19临床救治专家推荐意见临床实施简表」的推荐及说明
7465
2
翟振国教授|重症新冠患者的抗凝治疗:如何平衡血栓和出血的风险
6757
3
重症新冠病毒感染的呼吸支持治疗
4570
4
COVID-19炎症因子及免疫失衡指标&共感染
4228
5
重症COVID-19病例分享-2
3969
6
重症新冠合并感染的临床流行病学
3683
7
新冠病毒肺部感染影像学特征及动态演变
3556
8
我国Omicron变异株所致重症COVID-19的流行病学
3424
9
重症新冠肺炎的临床表现
3396
10
詹庆元教授:重症新冠感染救治的几个关键问题
3208


友情链接
联系我们
 公众号
公众号
 客服微信
客服微信